|
Historical informatics
Reference:
Danilov E.V.
Zemstvo medicine and healthcare seeking in the late 19th – early 20th centuries: evidence from Samara uezd
// Historical informatics.
2024. ą 1.
P. 37-55.
DOI: 10.7256/2585-7797.2024.1.70375 EDN: QAYQJB URL: https://en.nbpublish.com/library_read_article.php?id=70375
Zemstvo medicine and healthcare seeking in the late 19th – early 20th centuries: evidence from Samara uezd
Danilov Evgenii Vladimirovich
Postgraduate student, Department of Historical Information Science in Lomonosov Moscow State University
119991, Russia, Moscow, Lomonosovsky Prospekt, 27 bldg. 4, of. G-423

|
random.pc.user@gmail.com
|
|
 |
Other publications by this author
|
|
|
DOI: 10.7256/2585-7797.2024.1.70375
EDN: QAYQJB
Received:
04-04-2024
Published:
11-04-2024
Abstract:
This article examines the state of zemstvo medicine in Samara uezd in 1886–1913. An important aspect of this analysis is the study of healthcare seeking, which serves both as a statistical parameter of the frequency of medical care seeking and an indicator of very complex sociocultural dynamics within certain society. One’s decision to visit a hospital, and in general one’s perception of his or her own physical body and its deviations and abnormalities in medical terms are influenced by multiple factors that are not limited to the characteristics of the healthcare systems. Similar issues are studied in detail within the framework of medicalization, as well as the methodology of health seeking behavior, which examines the factors behind people’s decisions to follow healthy lifestyles, including visiting hospitals. This research is based on medical and statistical reports of the Samara uezd physicians in the late 19th – early 20th centuries and examines the temporal and spatial dynamics of the healthcare seeking; the main purpose of this study is to measure disparity levels of healthcare seeking practices in different parts of Samara uezd. Firstly, the study reveals that in the infrastructural aspect, healthcare in the Samara uezd was in an active development stage, which reflected in an increase in both the number of medical stations and hospitals, and physicians and paramedics. Secondly, the healthcare seeking rates was also evolved in a positive direction, which is reflected in an increase in both the number of medical services delivered to population. Furthermore, it shows the decrease of heterogeneity level of healthcare seeking rates between medical stations in uezd from 1898 to 1913; however, this level between the volosts remains high even after 15 years.
Keywords:
healthcare, Russian Empire, medical care, medicalization, physician, zemstvo, Samara, paramedic, healthcare seeking, history of medicine
This article is automatically translated.
You can find original text of the article here.
Problem statement At the turn of the XIX–XX centuries, Russia was in a state of active social and economic development, which echoed many aspects of public life in the country. Thus, this period was also marked by the rapid development of public medicine (especially zemstvo): frequent congresses of doctors, discussions on reforming the medical department, active construction of new hospitals. The established research tradition in the history of medicine is quite diverse: it presents both works devoted to the description of the organization and activities of medical institutions and figures [1-4], and more highly specialized (works devoted to the problems of the relationship and correlation of power and medicine [5; 6], medicine and society [7; 8], medicine and statistics [9; 10]. However, it is worth noting that the study of public medicine of the Russian Empire in the prism of statistical analysis remains quite inactive to this day. In this work, an attempt is made to study the functioning of zemstvo medicine on the example of the Samara district in the late XIX – early XX centuries. In many ways, it is a continuation of the work in which a study was conducted on how the level of public access to medical care was distributed and what factors influenced this process [11; 12]. The need for medical care was chosen as the subject of the study because it is an indicator of the interaction between healthcare and society: a person who is facing a problem with his health (or believes that he is), seeks medical help from medical institutions. But it may not apply – and this decision to (not) seek medical help is influenced by many factors of a very different nature. This work is largely based on the methodology of “healthy lifestyle models” (health seeking behavior), which generally explores the problems of people's behavior in relation to their own health: leading (not) a healthy lifestyle, applying to medical institutions, tactics for treating diseases and much more [13-16]. In particular, this umbrella area includes the topic of healthcare seeking behavior, which examines the factors that influence a person when making a decision to go to hospitals for medical care. In general, they can be defined as a set of socio-economic, cultural, geographical, and organizational factors that influence people's behavior in the issue of interaction with the field of scientific medicine [17; 18]. In the sociological dimension, this approach largely echoes the concept of medicalization, which arose in the second half of the 20th century [19, p. 21; 20] and assumed the involvement of people in contact with medicine, as well as the perception of their body and its deviations in medical optics. In a sense, this echoes Roy Porter's call to perceive the history of medicine not only as the history of doctors, hospitals and medical theories, but also as the history of patients themselves, their perception of their health and its deviations, relationships with doctors and scientific medicine in general [21]. One of the main works that study medicine from the point of view of its perception by patients in the Russian Empire is the work of Gabriel Ivanovich Popov “Russian folk medicine” [22]. Popov, based on the data of the “Ethnographic Bureau” of Prince V.N. Tenishev [23, pp. 274-275], summarized and analyzed information about the perception of the peasants of European Russia of problems related to their health: a separate chapter of this book is devoted to the attitude of peasants to scientific medicine. Popov's research suggests that the dynamics of the relationship between people and medicine is not limited exclusively to instrumental logic, that is, conditional availability of medical care, but is also formed under the influence of social and cultural factors [23, 276-277]. However, it should be noted that “Russian Folk Medicine” is an ethnographic and anthropological study, and the conclusions drawn in it, despite its enormous scientific value, would be wonderful to supplement with statistical estimates. In my research, attempts were made to assess the degree of uniformity of the distribution of the level of circulation: they showed that in European Russia, the level of circulation was largely unevenly distributed in the regions both at the provincial level [11] and at the county level [12]. In addition, with regard to the outpatient sector, assumptions were formulated that organizational and infrastructural factors did not have a dominant influence on the level of appeal, which is probably due to the influence of factors of a different nature: social, cultural, economic and others. Such an observation echoes Popov's work, although it is worth noting that the format of such a proof has a “contrary” character. This article presents an attempt to analyze the development of medicine in the Samara region at the turn of the XIX – early XX centuries through the prism of the evolution of the processes of circulation in it during this period. The main focus of the study is aimed at comparing and evaluating the extent to which the practice of seeking medical care in Samara County was widespread in different parts of it – among medical sites and municipalities. Data
This study is based on the information contained in the medical reports of the Samara County Zemstvo Council, issued in the 1880s - 1910s. These reports were collections of statistical information on the state of medicine and healthcare in Samara county. Each reporting year was reflected in a separate report, which were issued in the following reporting year. The report form changed over time: in the 1880s and 1890s, they mainly consisted of two conditional parts: from doctors' reports on the state of affairs for the reporting year in the medical stations to which they were attached, as well as a general summary of the county, which was compiled on the basis of district reports. However, by the beginning of the 20th century, the form had undergone changes: protocols and journals of meetings of county doctors were introduced into medical reports, at which organizational issues were often discussed: on payment of benefits, on the opening of new hospitals, on the working hours [24, p. 133], on business trips [24, p. 117], etc. The general summary included information on the characteristics of medical sites (their territorial location, number of population, medical staff), outpatient and inpatient admission, obstetric care and smallpox vaccination. The synthesis of these data is based on the use of a card system, the introduction of which into the process of medical practice was actively promoted at least in the field of zemstvo medicine (due to the great potential for spatial and socio-demographic analysis of the morbidity of the population [25, pp. 17-32], although it caused dissatisfaction due to its labor intensity – especially at the initial stage of its development introduction [26, pp. 99-105]). The cards were mostly filled out by doctors in outpatient clinics based on the accepted nomenclature of diseases, while in paramedic stations, paramedics filled out the cards only in case of admission of patients with infectious diseases. Inpatient hospitals (hospitals and reception rooms) also had a card system for recording patients. Information on each site was sent to the board at the beginning of the next reporting year [24]. The meaningful integrity of the reports can be described as follows. Over the rather long practice of publishing reports – since 1886 [27, p. 65] – the dynamics of the degree of filling of reports is quite noticeable. So, until the end of the 1890s, reports for the most part provided only the most basic information about the number of patients and the main parameters of medical sites, while the differentiation of these data was rather meager. For example, during this period, the separation of patient admission in outpatient clinics and paramedic stations was practically not observed, updated information about the paramedic stations themselves was not provided, there was no more detailed information about the admission of patients with their division according to the territorial (volost) principle – these gaps were largely filled in later reports. That is, in general, the structure of reports has become more complicated over time and the degree of their fullness has increased, which largely indicates the gradual nature of the development of reporting. The most valuable data for this study are the data on the infrastructural state of zemstvo medicine in the county (the number of medical sites and their characteristics) and the population's access to medical care – both outpatient and inpatient. This information, together with data on demography (based on the All-Russian Population Census[28]) and financing (contained in the reports of the Samara Zemstvo District Council [29-31]), allows us to form a characteristic of the processes of seeking medical care in the Samara district. Necessary remarks and design of the study Due to the fact that the level of referrals is calculated as the ratio of the number of requests for medical care to the population, it is necessary to make the following remark: the demographic information presented in the report is based on population movement calculations conducted by the board. If until 1897 it is not possible to accurately assess how reliable these calculations are, then based on the data of the General Census, this assessment can be made [28]. So, according to the medical report of Samara county for 1898, the county (excluding Samara) It was divided into 14 medical sites, in which 252 thousand people lived. At the same time, according to the General Population Census, the population of Samara county as of 1897 amounted to 267 thousand people, excluding Samara. This results in a discrepancy of 15 thousand (with a delay of one year), which is about 6% relative to the report data. The reason for this discrepancy remains unclear – however, such a difference in estimates is probably not a reason to categorically distrust the data of the medical report, which makes it possible to use them to calculate the level of circulation in the county. Probably, this also gives reason to relatively trust the demographic calculations of the county council for the following years, which were mainly formulated on the basis of population movement data, especially by 1913 – due to the fact that by 1913 a household census was conducted in Samara province, including in Samara County. The design of the study is as follows: from the entire period of 1886-1913, it was decided to analyze 2 time slices: for 1898 and 1913. This is due to the fact that in the reports for these years, data on circulation were included, dividing them not only by medical sites, but also by volosts – that is, this makes it possible to assess the level of circulation not only within the medical site, which may consist of several volosts and their parts, but also in the volost projection, that is, real settlements, about which there is demographic information.
First, a brief summary of the state of medical infrastructure in Samara County for 1886, 1898 and 1913 is given, followed by an analysis of the availability of medical care. The data on primary medical care requests are mainly analyzed both in outpatient clinics and in independent paramedic stations. In order to avoid confusion in the operation of these parameters, it was decided to encode them as follows: primary access to medical care in the outpatient clinic is presented in the form of outpatient access, primary access to medical care both in the outpatient clinic and in paramedic stations – in the form of general access. The decision to introduce such terminology is due to the fact that it seems incorrect to use the term “morbidity” in relation to primary admission due to the fact that primary applications indicate a detected morbidity rather than an approximate one, due to a relatively undeveloped culture to seek medical help in case of illness in pre-revolutionary Russia. Hospital visits are described in the work as stationary callability. The data on circulation are analyzed both in dynamics and in the prism of distribution over the territory of the Samara district. The latter is presented in the form of two projections: divisions according to the principle of medical sites and according to the volost principle. This division allows us to look at the dynamics of treatment not only within the medical sites, which are composed of several neighboring municipalities and in many ways give a fairly conditional idea of the practices of seeking medical care in real settlements, but also on the example of the municipalities themselves. Zemstvo medicine in the Samara district: characteristics In 1886, Samara County was divided into 9 medical districts. In each of these sites there was a medical outpatient clinic, in which outpatient appointments were carried out – mainly by a doctor, but also by paramedics at these outpatient clinics (including in the absence of a doctor). There were 3 zemstvo hospitals and 1 emergency room in the county, where inpatient patients were admitted. In addition, there were 16 paramedic stations, which also provided outpatient admission, these points were headed by paramedics. On average, there were 1,460 square versts per 1 medical site, which conditionally corresponds to a site radius of 21.5 versts (which is significantly higher than the recommended radius of 15 versts). In the county, admission of both inpatient and outpatient patients was carried out free of charge by 1886 (the free treatment status remained at least until 1898 [32, p. 71]), while financing went through the zemstvo board within the established estimates with mandatory reporting of doctors on expenses [27, p. 64-65]. In total, in 1886, about 113 thousand primary requests for medical care were made in Samara County: 61355 requests were accepted by doctors, 51748 requests were received by paramedics (unfortunately, it is difficult to determine which part of them was accepted by paramedics in an outpatient clinic, and which – in a paramedic station, due to the failure to provide data on this in the source). Also, in just one year, 748 inpatient patients were admitted, who spent a total of more than 15,000 days in the hospital. In total, 50,853 rubles were spent in 1886, provided by the county council – that is, the unit cost of one visit was about 45 kopecks. The situation had changed quite significantly by 1898. Thus, the number of medical stations has increased to 14, the number of paramedics has increased to 36 (of which 5 are in 5 paramedic stations). The average area of the medical site decreased to 940 square versts (the average radius is 17.3 versts), on average there were 18 thousand people per site (according to the population of the county council; about 19 thousand per site according to census data). In total, 162,380 people turned to doctors and paramedics in 1898, who made a total of 251,318 visits. Of these, 10,8889 people turned to doctors in outpatient clinics (174,228 visits), 23,334 people (34,571 visits) to paramedics, 30157 people (42519 visits) to paramedic stations. 1,176 people (who spent 9,600 days) were hospitalized in 3 hospitals and 1 emergency room with a total number of beds of 60 units. The total cost amounted to 92,508 rubles (with an estimate of 107850 rubles), which is about 37 kopecks per patient visit, and the specific cost of medical care for the population of the county is 37 kopecks per person (35 kopecks according to census data). By 1913, the infrastructural state of health care in Samara County was as follows: the number of medical sites increased to 20 (along with the site in Samara, which was opened to receive students from zemstvo schools, employees in the administration, as well as peasants located in the city [report for 1908]), and paramedics – 76 (10 of them they practiced in 8 paramedic stations). The average area of the medical site was 690 square versts (about 15 versts in radius for each site). On average, there were 18,445 people per site (according to the data on the population movement of the county council for 1913). In total, during the reporting year, there were 299,039 people in medical stations who made 508,627 visits. Of these, 239,273 patients were treated on an outpatient basis (who made 333,015 visits to doctors and 77,149 visits to paramedics), 59,766 people were admitted to paramedic stations (and made 98,463 visits). 4,163 people were treated inpatient in the county (who spent 50077 days in hospitals) in 3 hospitals and 11 reception rooms with a total number of beds of 120 units. In general, 252,315 rubles were spent on the medical part in the county (that is, the specific financing amounted to 72 kopecks per resident of the county). Fig. 1. The number of primary and repeated requests for medical care in Samara county, 1886-1913.
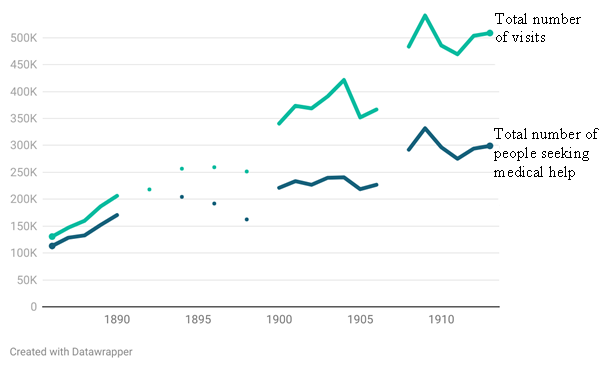
Sources: Report on ensuring public health in the Samara district in ... [by year, 1886-1913] / Samara Zemsky uyezd administration, 1887-1914. Note: Data gaps are due to the lack of sources. In general, from 1886 to 1913, the infrastructural potential of zemstvo medicine increased significantly – the number of medical stations and employees in them more than doubled. However, in stationary terms, this dynamics was not so linear: in the 1890s, there was a significant decrease in the number of hospitals and beds in them (which was due, among other things, to accidents in the form of fires, when in 1894 only one hospital operated in the entire county, with the exception of Samara due to a fire in the hospital of the Yekaterinovsky site), however, by the beginning of the 20th century, the potential of the inpatient sector began to grow again, which resulted in an increase in the number of hospitals and beds in them. The dynamics of the number of requests for medical care also took on a generally positive character: the number of primary applications in 1886-1913 increased by more than 2.5 times, and the total number of primary and repeated admissions increased by almost 4 times (Fig. 1); inpatient patients became more than 5 times more. However, the highest level of circulation in Samara County was observed in 1909, after which there was some decline; another decline, observed in the 1890s, is rather due to the lack of relevant data in the reports. It should also be borne in mind that there was a provincial zemstvo hospital in Samara, which, among other things, received residents of the Samara district, so it can be assumed that some of them sought medical help there (especially residents of neighboring Samara volosts). Medical treatment in Samara County: calculations and estimates In 1898, the circulation pattern in Samara County looked as follows: outpatient circulation amounted to 497.6 appeals per thousand people per year, and the total circulation rate reached 565.6 appeals within the entire county (Table 1). Thus, on average, almost every second resident of Samara County sought medical help in hospitals under the jurisdiction of the Samara County Zemstvo (however, this number also includes a certain proportion of residents of other counties and provinces). This indicator is averaged within the framework of 14 medical sites where patients were admitted. If we take into account the proportion of repeat visits, then the rates of treatment are modified as follows: outpatient treatment amounted to 828.5 visits per 1000 people, total – 997.2 visits. In many ways, these indicators are conditional due to the fact that they show an average estimate. If you look at the picture of how the level of appeal varies from site to site, the following composition is built. The highest level of outpatient referrals was observed in the Spassky medical district (806 primary referrals per 1,000 people), the lowest in the Koshkinsky district (323 primary referrals per 1,000 people). The standard deviation was 137 referrals per 1,000 people, which means that on average each site deviates from the average level of referrals by 137 units. The coefficient of variation in this case was 0.26 for primary outpatient treatment, which is the lowest in comparison with indicators of other parameters. If we take into account the admission in paramedic independent points, then the standard deviation increases to 273 units, and the coefficient of variation increases to 0.48. It turns out that when adding paramedic admission to the calculations of treatment, the level of uneven distribution of treatment between medical sites increases. That is, the presence of paramedic stations in the medical area increases the disparity in the level of access between the sites. Table 1. Descriptive statistics of medical treatment in Samara county, 1898 | | Outpatient treatment at medical sites | General circulation in medical areas | General circulation in the volosts | | Number of objects | 14 |
14 | 34 | | Average turnover, per 1000 people | 497,6 | 565,6 | 565,6 | | Minimum value | 323,8 | 435,4 | 122,1 | | Maximum value | 806,0 | 1072,9 | 1054,1 | | Standard deviation | 137,2 | 273,8 | 258,8 | | Coefficient of variation | 0,26 | 0,48 | 0,45 |
Source: Report on the provision of public health in the Samara district in 1898 / Samara Zemstvo District Council, 1899. This is largely due to the fact that paramedic stations were opened not only in areas with a low level of public access to medical care in outpatient clinics. For example, in the Chistovsky, Alekseevsky and Bogdanovsky precincts, where the level of outpatient referrals was in the range of 420-440 referrals per 1000 people, there was no paramedic station, while in the Yekaterinovsky and Krasnoyarsk precincts, where the level of outpatient referrals was above 600 units, paramedic stations were opened. The picture of the population's access to medical care in the projection of medical sites can also be compared with how the distribution of access looks at the level of municipalities. Thus, among the 34 volosts of the Samara district in 1898, there was a rather large unevenness in the distribution of referrals: residents of Chernorechenskaya volost applied for medical care the least intensively (122 applications per 1000 people), most of all – Tomylovskaya (1054 applications per 1000 people). However, the low level of appeal in the Chernorechensk region may be explained by its close geographical location to the city of Samara, which is why some residents could seek medical help in hospitals located there. In general, the coefficient of variation is 0.45, which indicates a fairly significant level of heterogeneity in how often residents of Samara County sought help in different parts of it – on average, in each parish there was a deviation in the level of appeal from the average for the county of 258.8 units. At the same time, the correlation coefficient between the level of treatment in the parish and the fact that a patient reception center is located in it is quite low (r = 0.4, p <0.05, a statistically significant relationship), which rather suggests that residents of municipalities that did not have an outpatient clinic or a paramedic station were prepared to go to hospitals located in other (most likely neighboring) volosts. However, if you pay attention to the scale diagram (Fig. 2), the following picture emerges: if there is a patient reception center in the parish, the level of treatment in it is more likely to be above average. On the other hand, in those volosts in which there is no reception point for patients, the intensity of treatment is much more diverse (including it is higher than in volosts with outpatient clinics and paramedic stations in them). Fig. 2. Diagram of the scope of medical care in the volosts of Samara county, 1898 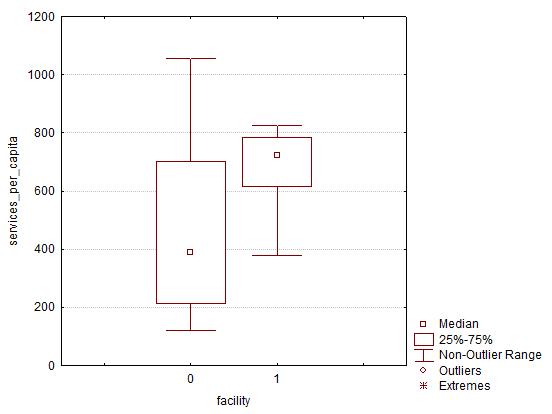
Source: Report on the provision of public health in the Samara district in 1898 / Samara Zemstvo District Council, 1899. Notes: on the vertical axis there is a scale of the level of medical care, on the horizontal axis there is the status of the presence of a patient reception point in the parish (0 – there is an admission point, 1 – there is no admission point). Such results may indicate the following. The level of treatment among medical sites was distributed relatively evenly when taking into account exclusively outpatient admission – when including in the model the proportion of admission carried out in paramedic stations, the level of heterogeneity increases significantly. That is, the presence of paramedic stations probably has an impact on the level of access in the medical area. At the same time, such heterogeneity is also characteristic of the ratio of the level of circulation among the municipalities, and the contribution to this heterogeneity is largely made by those municipalities in which there are no reception points for patients. By 1913, the pattern of medical treatment was transformed as follows. On average, the level of primary referrals in the outpatient clinic in Samara County has increased to 633.3 referrals per thousand people (if you add to this indicator the statistics of referrals in paramedic stations, the number of referrals increases to 801.7 units). At the same time, the highest level of outpatient and general referrals was observed in the Spassky district (919.9 and 1264.6 referrals per 1000 people, respectively), the lowest in Studenetsky (239.3) and Petropavlovsk (554.8) districts. It should be noted that in both variants, the coefficient of variation is 0.24 and 0.27, respectively, which indicates a relatively low level of heterogeneity in the distribution of access between medical sites. However, if we turn to the data on reversibility in the projection of the parish division, the picture changes somewhat. Thus, both outpatient and general referrals are characterized by higher coefficient of variation (0.45 and 0.42, respectively), which may indicate that during the transition from the precinct projection to the projection of the parish division, a relatively higher heterogeneity of medical care is observed. Table 2. Descriptive statistics of medical treatment in Samara county, 1913 |
| Outpatient treatment at medical sites | General appeal in medical areas | Outpatient treatment in the municipalities | General circulation in the municipalities | Stationary circulation in the municipalities | | Number of objects | 19* | 19* | 37 | 37 | 37 | | Average turnover, per 1000 people | 633,3 | 801,7 | 633,3 | 801,7 | 10,44 | | Minimum value | 239,3 | 554,8 | 96,1 | 213,7 |
0,25 | | Maximum value | 919,9 | 1264,6 | 1119,6 | 1730,3 | 38,61 | | Standard deviation | 164,4 | 216,6 | 284,1 | 339,0 | 7,88 | | Coefficient of variation | 0,24 | 0,27 | 0,45 | 0,42 | 0,75 | Source: Report on the provision of public health in the Samara district in 1913 / Samara Zemstvo District Council, 1914. Note: * – the table includes data on 19 medical sites with the exception of the site in Samara.
Was there some relationship between the level of treatment in the parish, as well as whether there is a patient reception point (outpatient clinic or paramedic station)? The correlation analysis showed that the level of correlation between these parameters is r = 0.52 (p <0.05, a statistically significant relationship), which indicates that there is some connection between the level of circulation in the parish and the presence of a patient reception point in it (which indicates the likely importance of the factor of the geographical location of the reception points). In general, the level of treatment is somewhat higher in those volosts in which an outpatient clinic or a paramedic station are located (Fig. 3). At the same time, the importance of having a paramedic station should not be underestimated: the proportion of admission of patients by paramedic stations averaged 67% of the total admission in those volosts in which these points were located (in the same volosts that do not have a paramedic station, the number of applications in them is negligible, and in the absence of an outpatient clinic in the volost, patients almost always applied to outpatient clinics in neighboring volosts rather than to paramedic stations). But even in those municipalities where there were reception points for patients, the level of referrals was largely unevenly distributed: the spread of the main part of the values ranged from 400 to 1400 with outliers exceeding the mark of 1600 referrals. This may indicate that there were some other factors in these municipalities that had an impact on the level of circulation, including those unrelated to infrastructural factors. Fig. 3. Diagram of the scope of medical care in the volosts of Samara county, 1913 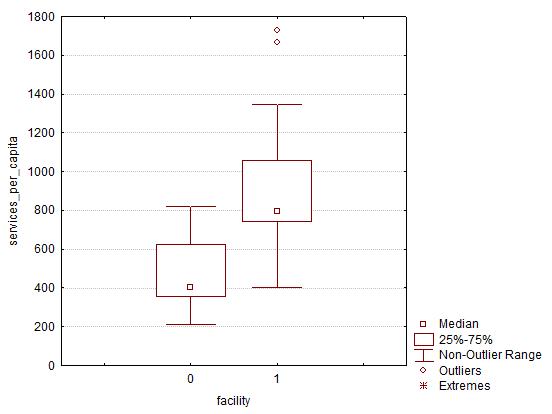
Source: Report on the provision of public health in the Samara district in 1913 / Samara Zemstvo District Council, 1914. Notes: on the vertical axis there is a scale of the level of medical care, on the horizontal axis there is the status of the presence of a patient reception point in the parish (0 – there is an admission point, 1 – there is no admission point). When comparing the results of the analysis of circulation in 1898 and 1913, the following observations can be distinguished. Firstly, in all calculation options, the level of medical care requests increased by 1913. This indicates the positive dynamics of the development of the practice of interaction between people and medical institutions. Secondly, in 1913, compared with 1898, the level of heterogeneity in the distribution of referrals between medical sites significantly decreased. This is especially significant on the example of general circulation: for example, if in 1898 the level of heterogeneity increased significantly when taking into account admission in paramedic stations relative only to outpatient admission, then by 1913 this difference had become noticeably less significant. That is, it can be assumed that by 1913 it was possible to ensure that the level of circulation between medical sites in the county was relatively uniform. However, the picture changes somewhat if we turn to the analysis in the projection of the parish division. Thus, the coefficient of variation is 0.45 and 0.42, which indicates that the level of circulation between the municipalities differed to a much greater extent than between medical sites. At the same time, the variation is similar to the observed heterogeneity in 1898. This may indicate that at the same time as the quantitative increase in circulation, the degree of its uneven distribution between the municipalities remained approximately at the same level. At the same time, it should be borne in mind that in 15 years 6 new sites were formed, and the number of paramedic stations increased from 5 to 8 (and 3 new municipalities were allocated). That is, it turns out that a quantitative increase in the level of circulation, as well as an increase in the infrastructural potential of zemstvo medicine, did not lead to a decrease in the level of inequality in terms of circulation between volosts. In addition, in 1898, the level of circulation in those volosts in which there were reception points for patients was more uniform than in 1913. If we look at the stationary sector of circulation, the picture appears as follows (Table 2). The average referral rate in 1913 was 10.44 inpatient patients per 1,000 people. At the same time, the minimum value was in the Voskresenskaya volost (0.25 – such a low indicator is probably due to the fact that the Voskresenskaya volost bordered Samara and a significant part of people sought medical care there), the maximum was in Yekaterinovskaya (38.61 – it is noteworthy that there was a hospital with 25 beds). A very high coefficient of variation is striking – 0.75, which indicates a high level of inequality between municipalities in terms of hospital admissions. However, there is a rather low correlation between this indicator and the fact that there is a hospital or an emergency room in the parish (r = 0.37, p <0.05, a statistically significant relationship). The scale diagram (Fig. 4) shows that, in general, in the volosts where hospitals are located, and in volosts without them, the level of hospital admissions is approximately commensurate – with an obvious outlier in the form of Yekaterinovskaya volost. It is noteworthy, however, that in Koshkinskaya volost, where there was also a hospital with 25 beds, the turnover was 20.6 inpatient patients per 1000 people, which is almost 2 times less. Fig. 4. Diagram of the scope of inpatient medical care in the volosts of Samara county, 1913
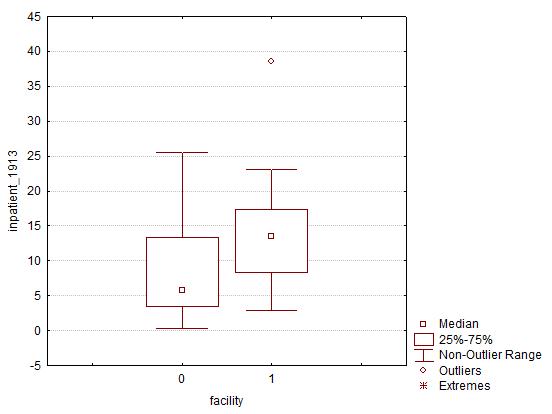
Source: Report on the provision of public health in the Samara district in 1913 / Samara Zemstvo District Council, 1914. Notes: on the vertical axis there is a scale of the level of inpatient medical care, on the horizontal axis there is the status of the presence of a hospital in the municipality (0 – there is a hospital, 1 – there is no hospital). Such a commensurate pattern of hospital admissions may be associated with a rather low level of baseline indicators, when the specific number of inpatient patients in the volosts rarely exceeded 20 patients per 1000 people (and in real numbers – several dozen people), and on such a scale, the importance of the geographical proximity factor may not play such an important role. Conclusions The results of the study can be presented in the following form. Firstly, during the period under study, the infrastructural potential of zemstvo medicine grew in Samara County as a whole, which was primarily reflected in an increase in the number of medical sites and medical personnel, as well as inpatient hospitals. At the same time, there was a positive trend in the number of requests for medical care. However, it would be premature to talk about a direct relationship between these parameters due to the fact that human interaction with medicine and healthcare is a complex multifactorial process. Secondly, the dynamics of the circulation level takes on a positive character: if in 1898 the average level of total circulation was 565 primary appeals per 1000 people, then by 1913 this figure exceeded the mark of 800 units. However, these are average indicators, which hide a significant heterogeneity in the manifestation of the circulation in different parts of the Samara district. Thus, in 1898, there was a certain uneven distribution of referrals among medical sites, which by 1913 had to some extent become more homogeneous. However, a rather high degree of heterogeneity was observed between the volosts both in 1898 and in 1913 – this is noteworthy against the background of the general increase in the number of patient reception points. This uneven nature can be explained to some extent by organizational and infrastructural factors; however, for a more complete understanding of the nature and mechanisms of the population's attitude to medicine and healthcare, an analysis using methodology from related disciplines: anthropology, sociology, psychology is required. This study is a continuation of an ongoing project dedicated to the study of the processes of seeking medical care in the Russian Empire at the turn of the XIX–XX centuries. In general, the results obtained are consistent with the available observations in the sense that the practice of seeking medical care in Samara County, as well as among counties and provinces of European Russia, is difficult to characterize as equally shared by all residents. However, it is difficult to assess to what extent these practices depend on the organizational and infrastructural state. The boundaries of medical sites have changed quite often, and it is quite difficult to compare demographic data (collected according to the principle of administrative division) and medical statistics (within the boundaries of medical sites), especially because of the discrepancy between these boundaries. However, such observations as the preservation of heterogeneity of circulation among the municipalities (and even among those in which there were reception points for patients) indicate a rather complex nature of the relationship between people and medical institutions. This, in turn, is one of the many indicators of the complex socio-cultural dynamics of Russian society at the turn of the century. Application Table 3. List of medical sites in 1898 | Medical area | Number of inhabitants | Plot status | Doctors | Paramedics |
| Koshkinsky | 27168 | Hospital, 25 beds, F.P. | V. F. Baykov | 4 | | Zubovsky | 26541 | Outpatient clinic | D. I. Gladyshev | 2 | | Kandabaluksky | 14277 | Outpatient clinic | Arkhangelsk | 2 | | Elshansky | 12989 | Outpatient clinic |
A. N. Voltman | 2 | | Elkhovsky | 22497 | Outpatient clinic, F.P. | I. O. Rachunas | 3 | | B. Kamensky | 12200 | Outpatient clinic | Bystrov | 2 | | Krasnoyarsk | 12306 | Outpatient clinic | N. F. Fastritsky | 3 | | Bogdanovsky |
21529 | Outpatient clinic | P. O. Efremov | 2 | | Alekseevsky | 20287 | Outpatient clinic | L. P. Kudryashev | 2 | | Dubovo-Umetsky | 14578 | Outpatient clinic | I. P. Troitsky | 2 | | Yekaterinovsky | 24000 | Hospital, 25 beds, F.P. | A. Goncharov |
4 | | Studenetsky | 14242 | Outpatient clinic, F.P. | I. G. Epstein | 3 | | Obsharovsky | 19000 | P.P., 5 beds | N. V. Farmakovsky | 2 | | Spassky | 10395 | Hospital, 10 beds | I. N. Gulyakov | 3 | Source: Report on the provision of public health in the Samara district in 1898 / Samara Zemstvo District Council, 1899. Note: P.P. – emergency room; F.P. – paramedic station Table 4. List of medical sites in 1913
| Medical area | The number of inhabitants of the site | Plot status | Doctors* | Paramedics | | Koshkinsky | 19201 | Hospital, 25 beds | P. V. Lebedev | 4 | | Chistovsky | 30028 | P.P., 5 beds, F.P. | The backup doctor | 4 | | Kandabaluksky | 15843 | P.P., 5 beds | A. I. Sungurov |
2 | | Elshansky | 20060 | P.P., 5 beds | L. A. Pavlovskaya | 2 | | Elkhovsky | 22148 | P.P., 5 beds | N. V. Farmakovsky | 3 | | Kamensky | 20267 | P.P., 5 beds, F.P. | A. Ya. Bystrov | 3 | | Krasnoyarsk | 17559 |
P.P., 5 beds | N. P. Chalovsky | 2 | | Bogdanovsky | 15157 | P.P., 5 beds | K. P. Muromtsev | 2 | | Alekseevsky | 14819 | P.P., 5 beds | I. P. Troitsky | 3 | | Dubovo-Umetsky | 14100 | P.P., 5 beds | M. A. Alfionov | 2 |
| Yekaterinovsky | 24095 | Hospital, 25 beds, F.P. | E. I. Sokolov | 5 | | Studenetsky | 20249 | Outpatient clinic, F.P. | The backup doctor | 4 | | Obsharovsky | 23515 | PP, 10 beds, F.P. | D. A. Goncharov | 4 | | Spassky | 14311 | Hospital, 10 beds, F.P. |
I. N. Gulyakov | 4 | | Stepno-Shentalinsky | 17991 | Item 5 beds | The backup doctor | 2 | | Samara | | Outpatient clinic, F.P. | L. P. Kudryashev | 3 | | Tomylovsky | 17112 | Outpatient clinic | A. I. Voronov | 2 | | Bobrovsky |
13608 | Outpatient clinic, F.P. | K. N. Edryshov | 3 | | Trostyansky | 13609 | Outpatient clinic | N. I. Leshchev | 2 | | Petropavlovsky | 16739 | Outpatient clinic | S. T. Velhover | 2 | Source: Report on the provision of public health in the Samara district in 1913 / Samara Zemstvo District Council, 1914. Notes: P.P. – emergency room; F.P. – paramedic station; * – data are given for 1912
References
1. Khabriev, R. (ed.) (2014. History of healthcare in pre-revolutionary Russia (late 19th – early 20th centuries). Moscow: GEOTAR-Media.
2. Mirskiy, M. (2005) Medicine in Russia in 10th – 20th centuries: essays on history. Moscow: ROSSPEN.
3. Smirnova, E. (2017). Formation of healthcare system in Russian province. 1775–1914 (on materials from the Upper Volga region). PhD dissertation. Yaroslavl.
4. Chernoukhov, D. (2020). Zemstvo medicine of the Perm province in the last third of the 19th – early 20th centuries. PhD dissertation. Yekaterinburg.
5. Hutchinson, J.F. (1990). Politics and public health in Revolutionary Russia, 1890–1918. Baltimore; London: The John Hopkins University Press.
6. Kuzmin, V. (2003). Power, society and zemstvo medicine (1864–1917). Samara: Samara University.
7. Bulgakova, L. A. (2011). «Mystery of zemstvo physician». Bulgakova, L. A. (Ed.). Medicine in Russia in war and peace times: new documents and studies. St. Petersburg: Nestor-History.
8. Pirogovskaya, M. (2018). Miasmata, Symptoms, and Evidence. Smells in Russian Culture, 1850–1900s: Between Medicine and Morals. Saint-Petersburg: European University Press.
9. Vishlenkova, E., Renner, A. (Eds.) (2021). The History of Medicine and Medical Geography in the Russian Empire. Moscow: Shiko.
10. Mitrofanov, R. (2023). «Her Language Must Be the Language of Figures». Medical Statistics of the Russian Empire and the Kingdom of Prussia: A Comparative Perspective, Quaestio Rossica, 11(2), 489-505. https://doi.org/10.15826/qr.2023.2.801
11. Danilov, E. (2022). Dynamics and factors of healthcare seeking in European Russia in early 20th century, Istoricheskaya informatika, 4, 65-83, available at: https://nbpublish.com/library_read_article.php?id=39251 (accessed: 23.06.2023).
12. Danilov, E. (2023). Zemstvo medicine and health care seeking in the late 19th century, Herald of Perm State University, 63(4), 148-160.
13. Evans, R. G., Stoddart, G. L. (1990). Producing health, consuming health care, Social Science & Medicine, 31(12), 1347-1363. doi:10.1016/0277-9536(90)90074-3
14. Andersen, R. M. (1995). Revisiting the Behavioral Model and Access to Medical Care: Does it Matter? Journal of Health and Social Behavior, 36(1), 1-10. doi:10.2307/2137284
15. Rahman, S.A. (2000). Utilization of primary health care services in rural Bangladesh: the population and provider perspectives. PhD dissertation. London: London School of Hygiene and Tropical Medicine, University of London.
16. Conner, M., Norman, P. (Eds.) (2005). Predicting Health Behaviour: Research and Practice with Social Cognition Models. Open University Press.
17. MacKian, S. (2003). A Review of Health Seeking Behaviour: Problems and Prospects. Internal Concept Paper Health Systems Development Program. London: London School of Hygiene and Tropical Medicine, University of London.
18. Zola, I. K. (1973). Pathways to the doctor – from person to patient, Social Science & Medicine, 7(9), 677-689.
19. Schlumbohm, J., Hagner, M., Sirotkina, I. (2008). «History of medicine: trends and prospects», in Schlumbohm, J., Hagner, M., Sirotkina, I. (Eds.). Illness and health: new approaches to the history of medicine. Saint-Petersburg: European University Press, 8–40.
20. Mikhel, D. (2011). Medicalization as social phenomenon, Herald of Saratov State Technical University, 4, 60(2), 256-263.
21. Porter, R. (2008). «A patient’s perspective, history of medicine», in Schlumbohm, J., Hagner, M., Sirotkina, I. (Eds.) Illness and health: new approaches to the history of medicine. Saint-Petersburg: European University Press, 41-72.
22. Popov, G.I. (1903). Russian folk medicine: review of materials from the Ethnographic Bureau of V.N. Tenishev. Saint-Petersburg: A.S. Suvorin Press.
23. Berger, E., Tutorskaya, M. (2023). Compliance in The Russian Village. Biopolitics or Dissemination of Hygiene Messages? Dialogue with time, 82, 272-285.
24. Lavrov, V.A. (1914). Report on public health provision in Samara uezd in 1913. Samara: L.M. Azerinsky Press.
25. Shingarev, A.I. (1906). Morbidity of Voronezh gubernia population, 1898–1902. General review of morbidity: based on card registration data. Voronezh.
26. Kapustin, M.Ya. (1889). Basic issues of zemstvo medicine. Saint-Petersburg: K.L. Rikker Press.
27. Zhbankov, D.N. (Ed.) (1893). Zemstvo medicine collection. Materials on the development of zemstvo medicine in Russia for the first 25 years (1865–1890). Vol. 4. Moscow.
28. Protopopov, I.A. (1900). List of populated places in Samara province. Samara.
29. Report of the Samara uezd zemstvo government for 1886. (1887). Samara.
30. Report of the Samara uezd zemstvo government for 1898. (1899). Samara.
31. Report of the Samara uezd zemstvo government for 1913. (1914). Samara.
32. Zemstvo medical activity review in 1898. (1902). Saint-Petersburg: Economic Department of the Ministry of Internal Affairs (3rd department).
Peer Review
Peer reviewers' evaluations remain confidential and are not disclosed to the public. Only external reviews, authorized for publication by the article's author(s), are made public. Typically, these final reviews are conducted after the manuscript's revision. Adhering to our double-blind review policy, the reviewer's identity is kept confidential.
The list of publisher reviewers can be found here.
The great reforms of Alexander II had such a great impact on Russian life that in pre-revolutionary historiography they even marked a watershed in the form of pre-reform and post-reform Russia. In modern Russia, in the context of the phased modernization of the healthcare system, it seems important to turn to the study of not only the Soviet, but also the pre-revolutionary experience of the formation of medicine. These circumstances determine the relevance of the article submitted for review, the subject of which is zemstvo medicine at the turn of the XIX - XX centuries. The author sets out to analyze the functioning of zemstvo medicine on the example of the Samara district in the late XIX – early XX centuries. The work is based on the principles of analysis and synthesis, reliability, objectivity, the methodological basis of the research is a systematic approach, which is based on the consideration of the object as an integral complex of interrelated elements. The scientific novelty of the article is determined by the very formulation of the topic: the author seeks to characterize zemstvo medicine and the availability of medical care at the turn of the XIX–XX centuries. using the example of statistical medical reports of the Samara district. Considering the bibliographic list of the article, its scale and versatility should be noted as a positive point: in total, the list of references includes over 30 different sources and studies, which in itself indicates the amount of preparatory work that its author has done. As noted above, the source base of the article is primarily represented by statistical data of zemstvo societies. From the studies used, we will point to the works of M.B. Mirsky, V.Yu. Kuzmin, M.Ya. Kapustin, which focus on various aspects of the study of the history of medicine in Russia. Note that the bibliography is important both from a scientific and educational point of view: after reading the text of the article, readers can turn to other materials on its topic. In general, in our opinion, the integrated use of various sources and research contributed to the solution of the tasks facing the author. The writing style of the article can be attributed to scientific, however, they are understandable not only to specialists, but also to a wide readership, to anyone interested in both the history of the healthcare system in Russia in general and zemstvo medicine in particular. The appeal to the opponents is presented at the level of the collected information received by the author during the work on the topic of the article. The structure of the work is characterized by a certain logic and consistency, it can be distinguished by an introduction, the main part, and conclusion. At the beginning, the author defines the relevance of the topic, shows that "the study of public medicine of the Russian Empire precisely in the prism of statistical analysis remains quite inactive to this day." The work shows that "during the period under study, the infrastructural potential of zemstvo medicine grew in Samara County as a whole, which was primarily expressed in an increase in the number of medical sites and medical personnel, as well as inpatient hospitals." The author notes that "the dynamics of the level of circulation takes on a positive character: if in 1898 the average level of total circulation was 565 primary appeals per 1000 people, then by 1913 this figure exceeded the mark of 800 units." It is noteworthy that, as the author of the reviewed article notes, "a fairly high degree of heterogeneity was observed between the volosts both in 1898 and in 1913 – this is noteworthy against the background of the general increase in the number of patient reception points." The main conclusion of the article is that "the results obtained are consistent with the available observations in the sense that the practice of seeking medical care in Samara County, as well as among counties and provinces of European Russia, is difficult to characterize as equally shared by all residents." The article submitted for review is devoted to an urgent topic, is provided with 4 figures and 4 tables, will arouse readers' interest, and its materials can be used both in lecture courses on the history of Russia and in various special courses. In general, in our opinion, the article can be recommended for publication in the journal "Historical Informatics".
|

 Eng
Eng









